The best diet plan for diabetes in India is not one plan. That is the first thing I want to say. Five years of seeing patients in my clinic in Patna has taught me that.
What works for a 52-year-old man in Lucknow is not the same as what works for a 38-year-old woman in Chennai. Region matters. Age matters. What your family eats matters.
I also want to talk about something that came out of a big ICMR study in 2025 that changed a few things in how I counsel patients now. More on that below.
If you read other blog about Fitness Tips for Beginners at Home
Back to the School Teacher
So I looked at her sheet. Dal, roti, rice, sabzi. Fine. But then I asked her how many rotis at lunch?
Four, she said.
And rice?
Two katoris.
Dal?
Half a katori.
There was the problem. Four rotis, two bowls of rice, and half a bowl of dal. The plate was about 85 percent carbohydrate. The one thing that could have balanced her blood sugar protein was barely there.
This is not unusual. This is most of my patients. Indian plates are carb-heavy by habit and tradition. That is not a personal failure. That is just how we were raised to eat.
I did not take away her rice. I did not take away her roti. I just shifted the portions. More dal. Less rice. One roti less at lunch. Walk 20 minutes after dinner.
Three months later her HbA1c was 7.9. She cried in my cabin. That was a good day.
If you read other blog about healthiest cooking oil in India
What the 2025 ICMR Study Found and Why It Matters to You
Late 2025. ICMR published the results of a survey covering over 18,000 adults across 30 Indian states. The study came out in Nature Medicine. I read through the key findings twice.
The main finding: Indians are getting about 62 percent of their daily calories from carbohydrates. Mostly white rice in the south and east. Wheat in the north. Sugar on top of both.
And this carb-heavy eating was linked to a 15 to 30 percent higher risk of type 2 diabetes, prediabetes, and obesity.
Here is the part that even surprised me a little. Just switching from white rice to whole wheat atta or millets did not reduce risk on its own.
The total amount of carbohydrate still being high was what drove the numbers. You cannot just swap the grain and think you are done.
What did reduce risk? Replacing some of those carb calories with protein. Dal. Rajma. Curd. Paneer. Eggs for non-vegetarians. That substitution made a real difference in the data.
I was not shocked by this. My patients had been showing me this for years. But having national survey data behind it makes the conversation easier. Now when a patient pushes back, I can say it is not just me telling you this.
What I Actually Put on a Patient’s Daily Plan
No two plans are identical in my clinic. Kidney function, cholesterol, weight, medications all of it changes things. But the base structure looks like this for most type 2 diabetic patients:
6:30 AM Before Anything Else
- 1 glass lukewarm water. Methi seeds soaked overnight strained and drunk, not eaten.
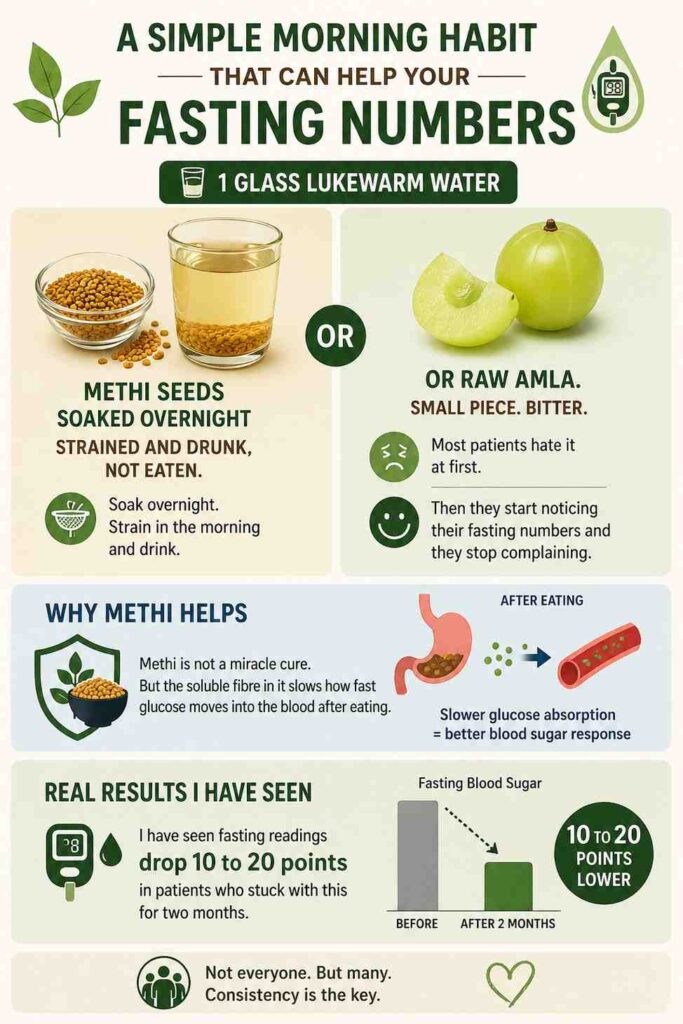
- Or raw amla. Small piece. Bitter. Most patients hate it at first. Then they start noticing their fasting numbers and they stop complaining.
Methi is not a miracle cure. But the soluble fibre in it slows how fast glucose moves into the blood after eating.
I have seen fasting readings drop 10 to 20 points in patients who stuck with this for two months. Not everyone. But many.
8 to 9 AM Breakfast
- 2 small ragi rotis with any dry sabzi this is my first recommendation for most North Indian patients
- Or moong dal chilla, 2 pieces, with green chutney
- Or oats upma with vegetables. Not sweet oats. Savoury.
- One boiled egg if non-vegetarian. Adds protein without adding carbs.

Ragi is my go-to because North Indian patients know it and can find it. Research from NIN confirms the glycemic index of ragi preparations sits between 54 and 68, which is significantly lower than a white bread slice at 75 or above. It also has calcium, which most of my patients are not getting enough of.
11 AM – Small Snack
- One guava. Or one apple. Eat the fruit. Do not juice it.
- Or a handful of roasted chana. Unsalted.
Almost every patient I see is skipping this snack. They think eating less means better sugar control. It does not.
When you go too long without eating, the liver dumps stored glucose into the blood on its own. That is what causes the strange spikes patients get on days they eat very little.
1 to 2 PM – Lunch
- 1 to 2 small rotis. Jowar or bajra if possible. Whole wheat if not.
- 1 full katori of dal. Not half. Full.
- 1 katori of sabzi. Preferably lauki, tinda, palak, or karela.
- 1 small bowl of plain curd. No sugar added.
- If having rice: half katori, brown or hand-pounded, not daily.
The dal is not optional. This is where the protein shift actually happens. Dal and a millet roti together is one of the most complete, blood-sugar-friendly meal combinations in Indian cooking.
It is already in our food culture. We just do not eat enough of it compared to the carb.
4 to 5 PM – Evening
- Plain buttermilk. No salt, no masala. Just chaas.
- Or green tea without sugar.
- 4 to 5 walnut halves. Or a small handful of pumpkin seeds.
Evening is the worst time for most of my patients. Chai with two spoons of sugar and biscuits. Three times a day.
That alone is six spoons of sugar most people are not counting. Replacing this slot with chaas and a few walnuts is one of the highest-impact swaps I recommend. It is not glamorous. It works.
7 to 7:30 PM – Dinner. Not Later.
- 1 small roti. Whole wheat or millet blend.
- 1 katori light dal or vegetable soup.
- 1 katori sabzi, lightly cooked.
- No rice at dinner for most patients. At least not in the first three months.
I am very firm on the dinner timing. Patients who eat dinner at 9 or 10 PM consistently show worse fasting readings the next morning.
The body handles glucose less efficiently late at night. Eating at 7 or 7:30 PM and walking even 15 minutes after can shift fasting numbers by 10 to 15 points in many patients. I have seen it too many times to be flexible on this one.
Mistakes I Correct Every Single Week
Five years. Same mistakes, different patients. Here are the ones that come up most:
- Fresh fruit juice. One glass of fresh orange juice has nearly the same blood sugar impact as a cold drink. The fibre is gone. The sugar hits fast. Eat the orange. Do not juice it.
- Multigrain or atta biscuits. Patients bring me packets thinking they made a good swap from regular biscuits. The refining process means the glycemic impact is still high. Biscuit is biscuit in my clinic.

- Eating very little to control sugar. Skipping meals does not lower blood sugar. The liver releases its own stored glucose when you go too long without eating. Many patients are actually spiking because they are eating too little, not too much.
- Not counting chai. Three cups of chai daily with two spoons of sugar each. That is six spoons. Before dinner. Hidden. Most patients have no idea they are doing it until I ask them to write it down.
- Thinking jaggery is safe. This comes up every week. Jaggery raises blood sugar at almost the same rate as white sugar. It has slightly more minerals. Not enough to make a clinical difference. Limit both.
What I Want You to Take From This
Managing diabetes through food in India is hard. Not because good food is unavailable. It is very available. Dal, curd, sabzi, millet roti all of it is already in our kitchens.
The problem is proportion. Too much carb. Not enough protein. Meals that are mostly starch and very little of anything else.
Shift the proportion. Eat more dal. Eat one less roti. Eat dinner before 8. Walk after meals. Drink water. These are not dramatic lifestyle overhauls. They are small adjustments that, done consistently, actually move the HbA1c.
I have watched patients bring their HbA1c from 10 down to under 7 without changing their medication. Only food and timing. It is possible. But it takes three months of actual consistency, not three days.
One last thing. Please do not use this article as a replacement for seeing a dietician who knows your full health picture. Kidney function, thyroid, other medications — these change what I recommend. This is a starting point, not a finished plan.
Can a diabetic patient eat rice?
Yes. Half a katori at lunch, paired with dal and sabzi. Not two katoris. Not at dinner every night. The problem is never the food — it is the amount and what it is eaten with. Rice alone on a plate spikes sugar. Rice with dal and a vegetable does not spike nearly as much because the protein and fibre slow the absorption down.
Which millet is best for diabetes?
Ragi, jowar, and bajra are all good. Ragi has the most calcium and fibre. Jowar I recommend more for patients who also have cholesterol issues. Bajra is better in winter. But honestly, rotating between them is better than picking one and sticking to it forever. Variety gives different nutrients. I do not have a single winner.
How many rotis can a diabetic eat in a day?
Three to four small rotis across all meals. Not three at one sitting. The distribution matters. One at breakfast, one or two at lunch, one at dinner. And always with protein alongside it. A roti eaten alone hits the blood sugar differently than a roti eaten with dal.
Can diabetics eat fruits?
Yes. Guava, jamun, amla, apple, and papaya in small portions are fine. Whole fruit, not juice. Between meals, not at the end of a big lunch. Mango, banana, and chikoo are higher in sugar — once in a while is okay but not daily and not in large amounts.
Does walking actually help blood sugar?
Yes, and faster than most patients expect. A 20-minute walk after the biggest meal of the day uses up blood glucose that is circulating at that point. I have patients who added only an evening walk and saw their post-meal readings drop by 20 to 30 points within weeks. Without any medicine change. Just the walk.